Mild · Grade I
Circumareolar (donut)
Confines the scar to the border of the areola. Suited to mild ptosis where only a small lift is combined with the implant.
Breast Surgery · Abu Dhabi & Dubai
Augmentation-mastopexy solves two problems in one operation: it lifts and reshapes a sagging breast and restores lost volume with an implant. Most patients have it as a single operation — the implant placed in a dual plane, the lift supported by an internal bra of your own tissue.

Overview
An augmentation-mastopexy combines two procedures in one: a mastopexy that raises the nipple, reshapes the breast and tightens stretched skin, and a breast augmentation that restores fullness with an implant. It is the answer when a breast is both sagging and deflated — the classic change after pregnancy, breastfeeding or weight loss.
A lift alone reshapes but adds no volume; an implant alone on a sagging breast only makes it hang lower. Done together, the lift positions and tightens while the implant fills the upper pole — a firmer, fuller, naturally-shaped breast.
In the vast majority of cases this is a single operation. The lift is then supported for the long term by an internal bra made from your own tissue, so it carries the implant without dropping again.
Why both are needed
A lift and an implant do two completely different jobs. When the breast has lost both position and volume, one alone cannot fix it — and choosing the wrong one is the commonest reason results look unnatural.
| Lift only | Implant only | Lift + implant | |
|---|---|---|---|
| Raises the nipple & tightens skin | Yes | No | Yes |
| Adds fullness & cup size | No | Yes | Yes |
| Right for a breast that sags and is empty | No — adds no volume | No — hangs lower | Yes |
| Best for | Sagging, still has volume | Good position, wants size | Sagging and deflated |
The “rock in a sock”
If the nipple already sits at or below the crease, adding an implant without a lift just pushes a heavy, low-hanging breast further down — the “rock in a sock” look. The skin must be tightened and the nipple raised at the same time as the volume is added. That is exactly what an augmentation-mastopexy does.
The starting point
The decision comes down to where your nipple sits relative to the inframammary crease. Dr. Paulo Michels maps this with the Regnault classification and standardized measurements — honestly, at consultation.
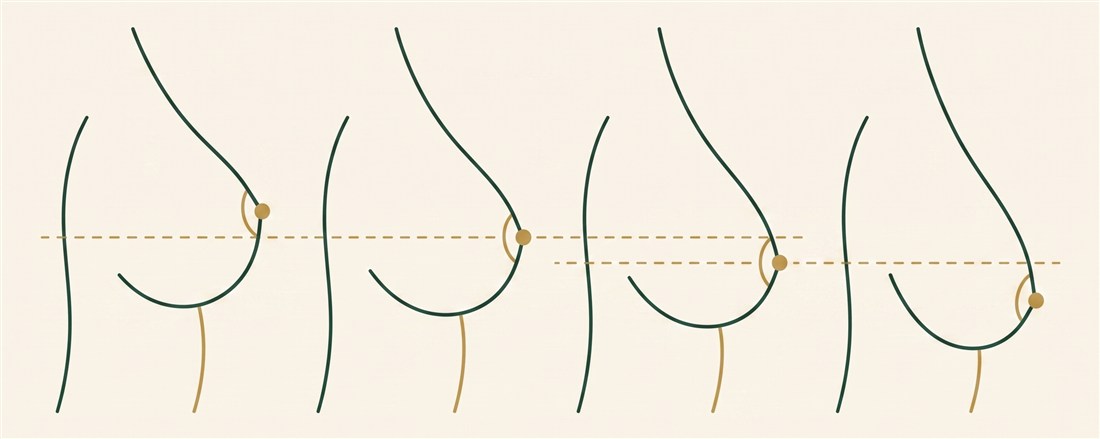
The lower pole is empty but the nipple stays above the crease. Often an implant (or a hybrid) alone restores shape — a full lift may not be needed.
The nipple sits slightly below the crease. A small lift is combined with the implant, usually through a limited scar.
The nipple sits 1–3 cm below the crease. A clear candidate for lift + implant together.
Pronounced sagging, nipple at the lowest point. Needs a full lift with the implant to restore height and fullness.
The honest test
If your nipple points down or sits below the fold, an implant alone will disappoint — you need the lift too. If it still sits above the fold and only the volume is gone, you may not need a full lift at all. The measurements make this an objective decision, not a guess — and you are always told honestly which operation your anatomy needs.
Single-stage vs staged
For most patients it is one operation. Dividing it into two stages is reserved for the specific situations where that is genuinely safer — never as a routine.
The lift and the implant are performed together in a single procedure and a single recovery. Careful planning — a controlled implant volume in a dual plane, matched to the tightened skin — lets both be done safely at once for the great majority of patients.
The operation is staged — lift first, implant once the tissues have healed and settled — when you want a notably larger implant that freshly lifted skin could not safely carry in one go, or when factors such as very thin skin, previous scarring or smoking raise the healing risk. A second, smaller operation buys a safer, more controlled result in exactly the cases that need it.
How the size is decided
Because the lift tightens the skin while the implant pushes outward, the two work against each other mechanically. So the default is a moderate, controlled implant in a dual plane — enough to restore upper-pole fullness without overloading the lift. If you want more volume, your measured anatomy decides whether the tissue can safely carry a larger implant — and when the size you want is more than a single-stage lift can hold, that is precisely when the operation is staged.
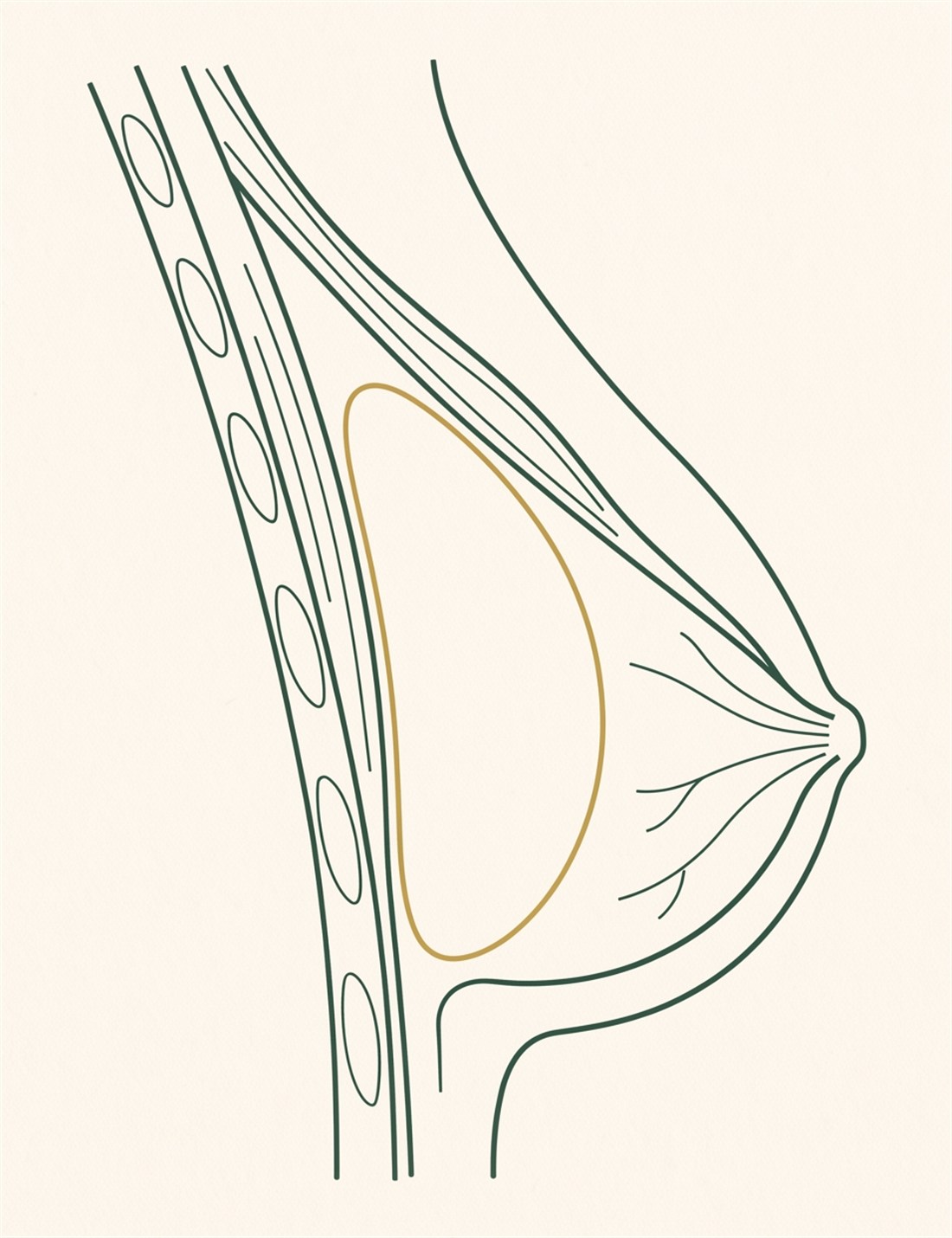
The pocket
In an augmentation-mastopexy the implant is placed in a dual plane: its upper part sits under the pectoralis muscle, its lower part behind the breast tissue. The muscle camouflages the top edge for a smooth, sloped upper pole, while the lower breast is free to be reshaped and lifted around it.
This matters more here than in a straightforward augmentation: the dual plane protects the implant against visibility and rippling in skin that has already been stretched and thinned, and gives the most reliable long-term support once the breast is lifted over it.
Placement, volume and profile are chosen from your measurements and a 3D simulation — so the fullness is planned before theatre, not guessed.
Planning
With two changes happening at once — the breast lifted and an implant added — 3D imaging is especially valuable. Your breasts are captured and the combined result previewed on your own body: the raised nipple, the tightened skin and the restored upper-pole fullness, together.
You can compare different implant volumes on the lifted breast and see how each looks, which makes the size decision shared and clear. Because a controlled volume protects the lift, the simulation helps you find the fullness you want within what your tissue can safely carry — and shows when a larger implant would be better staged.
With measurements and a careful examination, the plan becomes predictable and personal — lift and volume decided before theatre, not guessed.
3D simulation — what it gives you

Our philosophy
Why it lasts
A lifted breast that also holds an implant has more weight to support. Dr. Paulo Michels reinforces it with an internal support built from your own tissue — not a synthetic mesh.
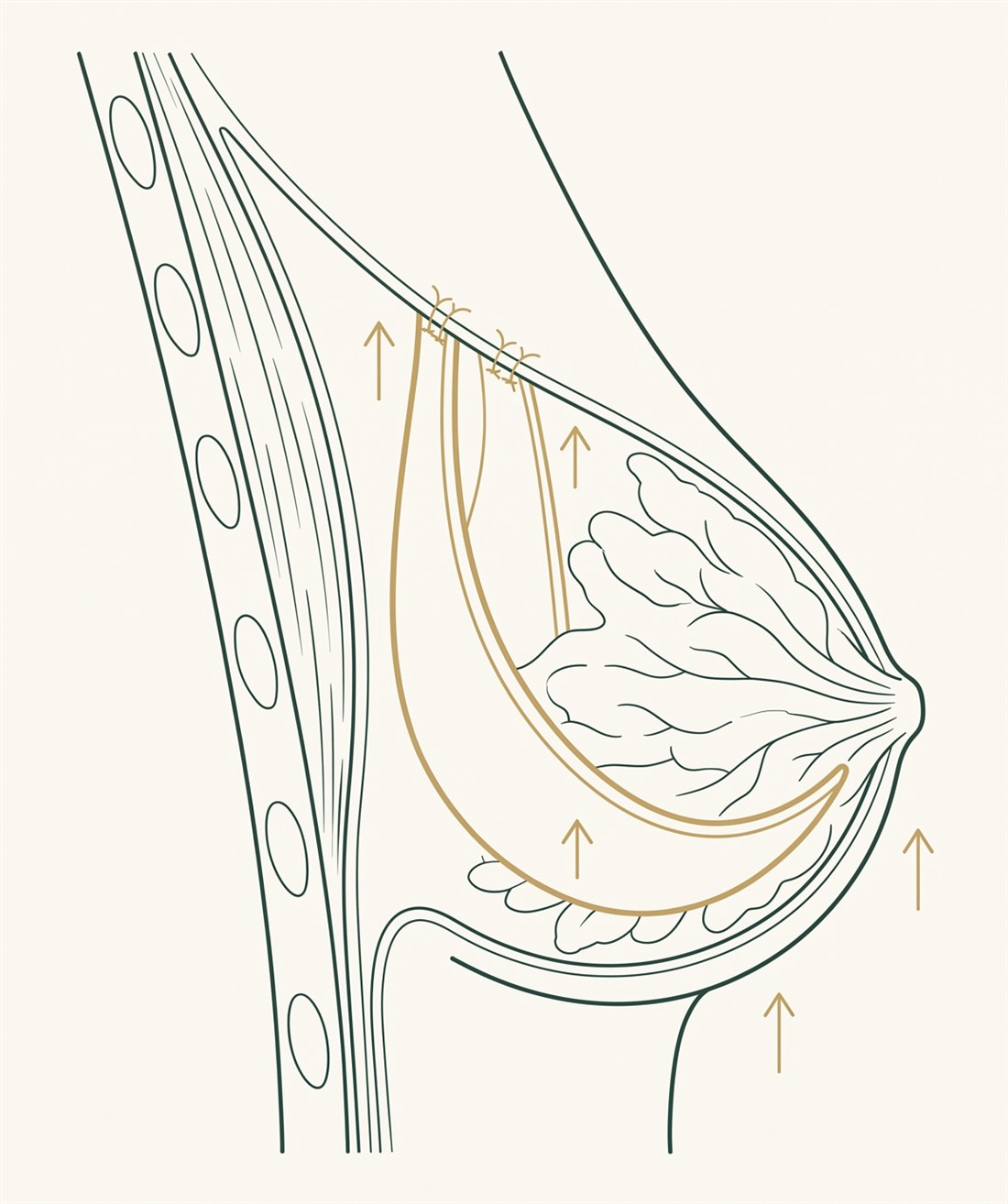
The inframammary fold — the crease that carries the weight of the breast and now the implant too — is reinforced using your own tissue. This creates a strong internal support that holds the breast up from below and resists the implant bottoming out or the lift dropping again over time.
Because the support is autologous — entirely your own tissue — there is no synthetic mesh, and therefore no risk of rejection or a foreign-body reaction. It is natural, durable support that becomes part of your own anatomy.
Matched to your ptosis
The incision is chosen entirely by your ptosis grade and how much skin must be removed — the least scarring that will still lift the breast and place the implant. The implant is inserted through the same incision, with no extra scar.
Mild · Grade I
Confines the scar to the border of the areola. Suited to mild ptosis where only a small lift is combined with the implant.
Moderate · Grade II
A circle around the areola plus a short vertical limb to the fold — firmer reshaping for moderate ptosis, and a common pattern for the combination.
Moderate–severe
Extends the lower incision only toward the outer side of the fold — removing more skin while keeping the central cleavage completely free of any scar.
Severe · Grade III
A periareolar circle, a vertical limb and a horizontal incision in the fold — for maximum reshaping when sagging is severe and the implant must be fully supported.
Nipple & areola
As part of every lift the nipple is repositioned to a natural height over the new fullness, and a stretched areola is reduced to a proportionate size — both through the same incision, with no additional scar.
Comfort & healing
The experience is engineered to be comfortable and to heal into the finest possible scar.
Modern anaesthesia
Complete, safe unconsciousness without inhaled gases — precise control, a smooth and rapid wake-up, and near-zero postoperative nausea, so you recover clear-headed and comfortable.
Pain-free wake-up
Targeted nerve blocks placed under ultrasound while you are asleep numb the chest-wall nerves, so you wake with zero surgical pain — sharply reducing strong painkillers and speeding your return to normal life.
Refined closure
Advanced surgical glue with a stabilising tape distributes tension evenly to prevent scar widening, for a remarkably thin line. It is 100% waterproof — early showering, no complex dressings and no external stitches.
Book a private consultation with Dr. Paulo Michels — an honest assessment of your ptosis, your tissue and whether a lift, an implant, or both together is right for you, in one operation or two.
Recovery
Recovery mirrors a breast lift: the nerve blocks and glued, stitch-free closure make the first days far easier than most expect. Most people return to work at around two weeks, with a supportive surgical bra worn for two months.
You wake with no surgical pain from the nerve blocks. You rest with the chest supported; the waterproof closure lets you shower early. Discomfort is mild and easily managed.
Swelling and tightness settle. You wear a supportive surgical bra day and night and avoid raising the arms forcefully. Most daily activities resume gently.
Most people return to desk work at around two weeks (14 days), depending on how physical the job is.
The surgical support bra is worn for two months to protect the shape, the implant position and the inframammary support as they heal.
Light activity builds back gradually; full exercise and chest or upper-body training resume at around three weeks (20 days). The breast settles into its final shape over 3–6 months as the implant drops and the swelling resolves.
Candidacy
Good to know
Honest risks
Augmentation-mastopexy is a safe, well-established operation, but combining a lift with an implant carries honest trade-offs: permanent scars (placed discreetly and refined to fade), temporary changes in nipple or skin sensation that usually recover, implant-related considerations shared with any augmentation, and the normal healing risks — slightly higher than a lift alone, which is exactly why size is planned conservatively and, when needed, the operation is staged. Everything is discussed fully at your consultation.
Patient stories
“After breastfeeding my breasts were empty and low. He lifted and added a modest implant in one operation — full and natural, not fake.”Lift + implant, single stage
“I wanted bigger, but he explained honestly it was safer to do the lift first and the larger implant after. So glad I trusted the plan.”Staged augmentation-mastopexy
“Zero pain waking up, no stitches to remove, and the scar sits only around the areola. The upper fullness is exactly what I missed.”Dual-plane, donut lift
Investment
Every breast is different, so there is no single price. A personalised quotation follows an in-person assessment. The main factors:
In line with UAE medical-advertising regulations, prices are shared privately in consultation rather than published.
FAQ
It is a breast lift and a breast augmentation performed together: the lift raises the nipple, reshapes the breast and tightens stretched skin, while an implant restores volume and upper-pole fullness. It is used when the breast is both sagging and deflated, typically after pregnancy, breastfeeding or weight loss.
It depends on where your nipple sits relative to the inframammary crease. If it sits at or below the fold, an implant alone will only hang lower (the “rock in a sock”) and you need a lift too. If the nipple is still above the fold and only volume is missing, an implant or hybrid alone may be enough. Measurements make this an objective decision.
For most patients it is a single operation. It is staged — lift first, implant once the tissues have healed — only in specific situations: when you want a notably larger implant that freshly lifted skin could not safely carry at once, or when factors such as very thin skin, previous scarring or smoking raise the healing risk.
Because an implant adds volume but does not raise the nipple or tighten skin. Placed under a sagging breast it simply pushes a heavy, low breast further down. The skin has to be tightened and the nipple lifted at the same time as the volume is added — which is what the combination does.
The default is a moderate, controlled implant in a dual plane, because the lift tightens the skin while the implant pushes outward and the two must be balanced. Your measured anatomy decides whether a larger implant can be carried safely; when the size you want is more than a single-stage lift can hold, the operation is staged.
In a dual plane — the upper part under the pectoralis muscle, the lower part behind the breast tissue. This camouflages the top edge for a smooth upper pole and protects against rippling in skin that has been stretched, giving the most reliable long-term support once the breast is lifted over it.
The scar follows your ptosis grade: a circumareolar (donut) scar for mild sagging, a vertical (lollipop) for moderate, and an L-scar or anchor (inverted-T) for severe. The L-scar keeps the central cleavage scar-free. The implant is inserted through the same incision, so it adds no extra scar.
It is an internal support made from your own tissue that reinforces the inframammary fold — the crease carrying the weight of the breast and now the implant — holding everything up from below. Because it uses no synthetic mesh there is no risk of rejection, and it helps the result last rather than bottoming out.
Most patients wake with zero surgical pain thanks to ultrasound-guided PECS nerve blocks placed during surgery, combined with modern TIVA anaesthesia that gives a smooth wake-up and almost no nausea.
It mirrors a breast lift: most people return to desk work at around two weeks (14 days), wear a supportive surgical bra for two months, and resume full physical and upper-body exercise at around three weeks (20 days). The breast settles into its final shape over three to six months.
Often, yes. The technique preserves the connection between the nipple and the milk ducts wherever possible, so many women can still breastfeed, though it cannot be guaranteed. Because a future pregnancy can re-stretch the breast, it is generally best to complete your family first. Tell Dr. Paulo Michels if breastfeeding matters so the plan accounts for it.
The result is long-lasting, especially reinforced with the inframammary support of your own tissue, which resists the lift dropping or the implant bottoming out. Ageing, large weight changes and pregnancy still affect the breast over time, so a stable weight and good support help it last.
Yes. An augmentation-mastopexy is commonly planned as part of a “mommy makeover” alongside a tummy tuck and liposuction, in a single anaesthetic and recovery. Suitability depends on your health and total operating time, and is decided at consultation.
Enquiry
Leave your details and Dr. Paulo Michels’ team will reply personally — or message on WhatsApp.