Will my breast implants look natural?
Yes — when the implant respects your anatomy. A personalised measurement system and 3D simulation select an implant that fits your chest precisely, placed in a dual plane for a smooth, sloped upper pole. The philosophy is elegant and proportional, never over-filled.
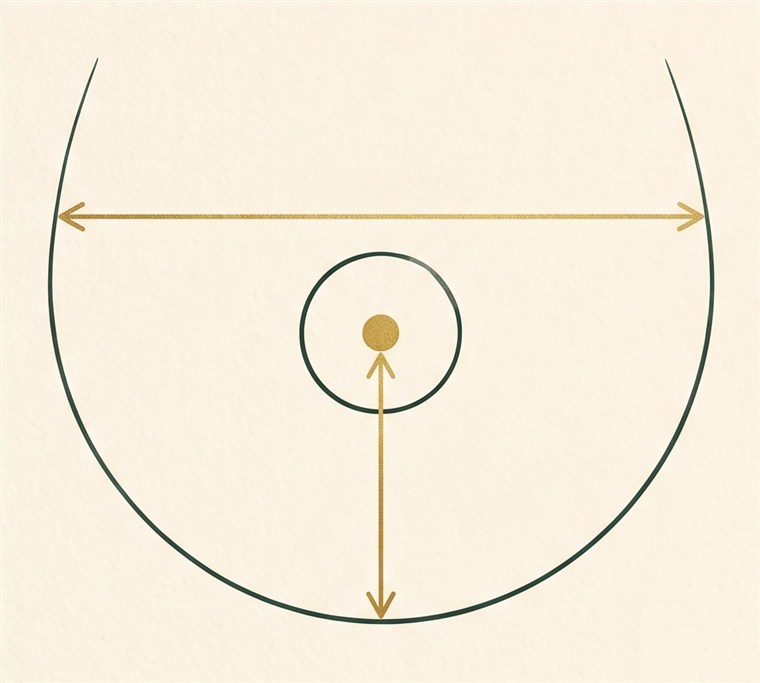
How do I choose my implant size?
By measurement and simulation, not guesswork. Your breast base width and tissue thickness define the safe range; 3D imaging then shows realistic previews of different volumes on your own body. As a rough guide, 150–200 cc is about one cup size.
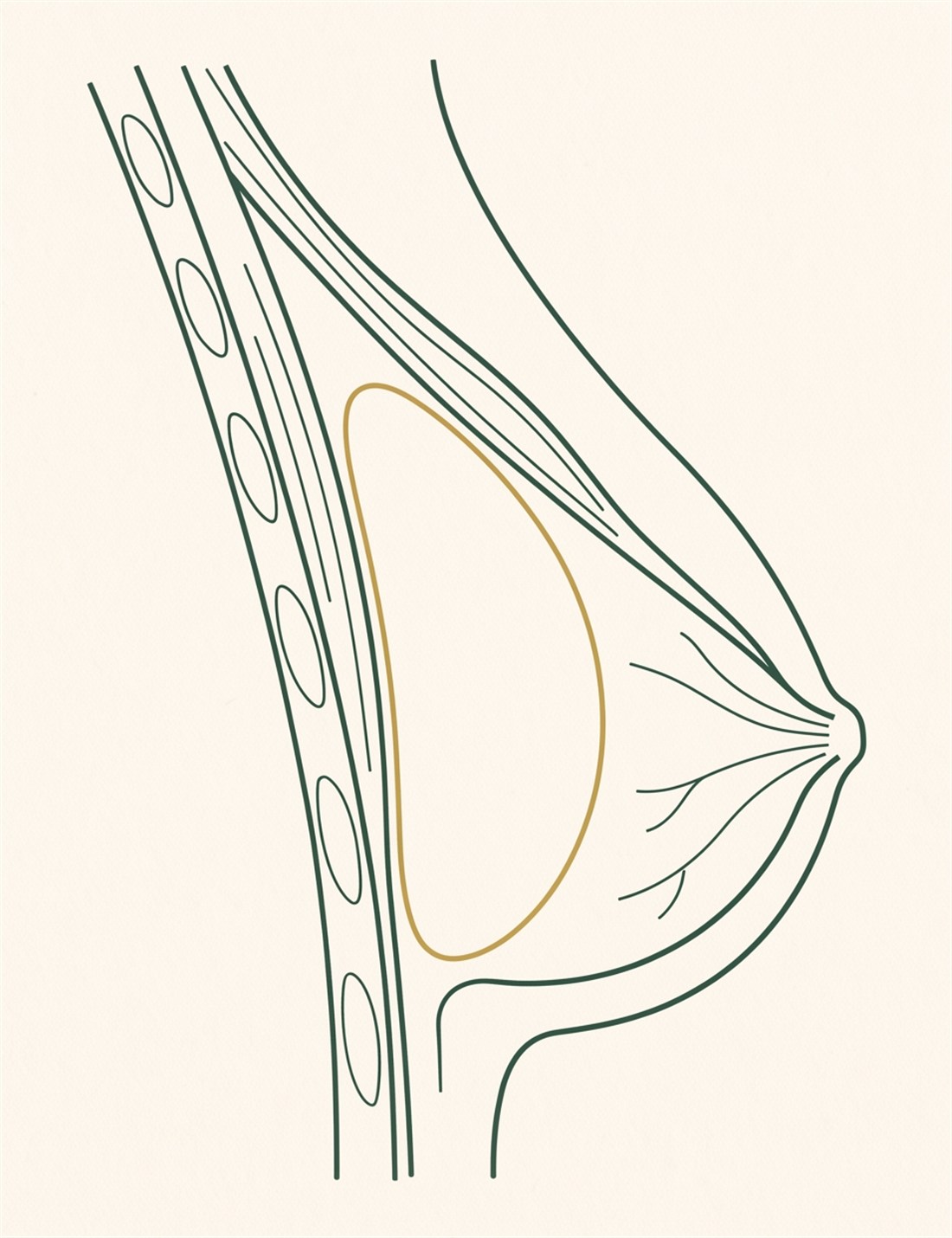
What is dual plane breast augmentation?
Dual plane places the upper part of the implant under the pectoralis muscle and the lower part behind the breast tissue. It combines muscle camouflage of the upper pole (no artificial shelf) with natural shaping of the lower pole — the reference technique for natural-looking results.
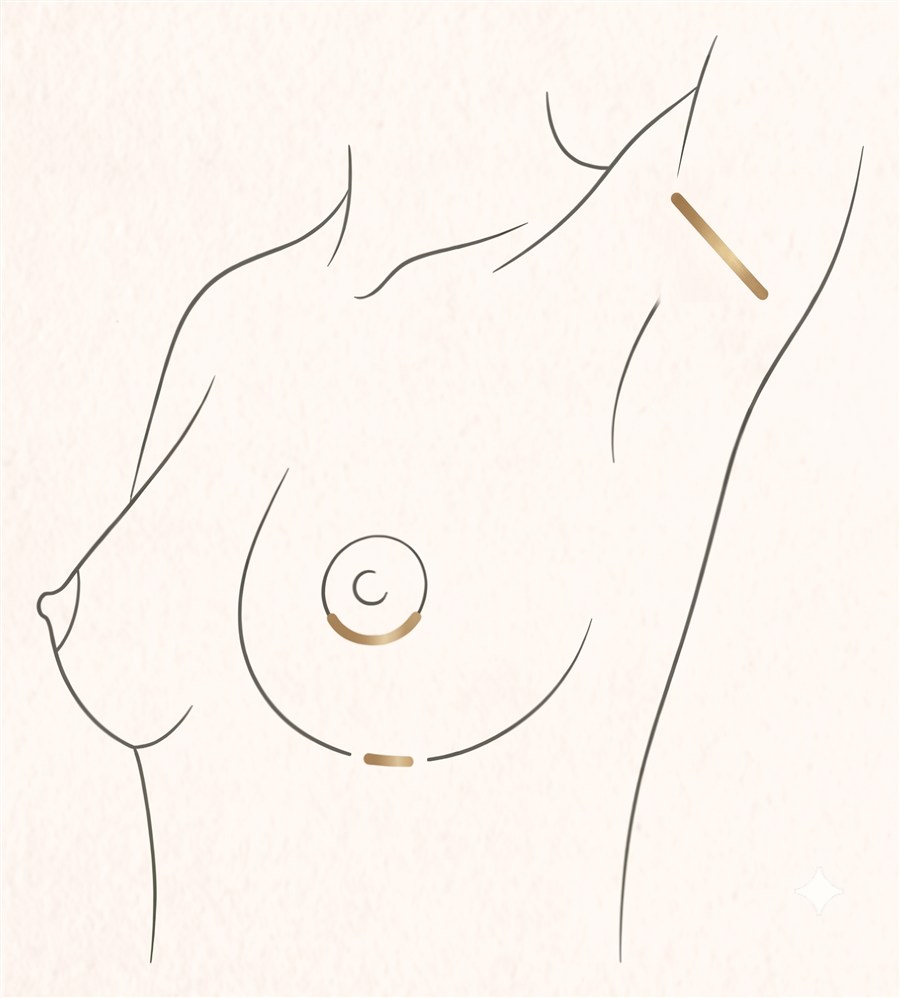
Where will my scar be?
In most cases a 2–3 cm incision hidden in the fold under the breast (inframammary), invisible in bras and bikinis. Closed with layered sutures and surgical glue, it typically matures into a fine, discreet line within 12–18 months.
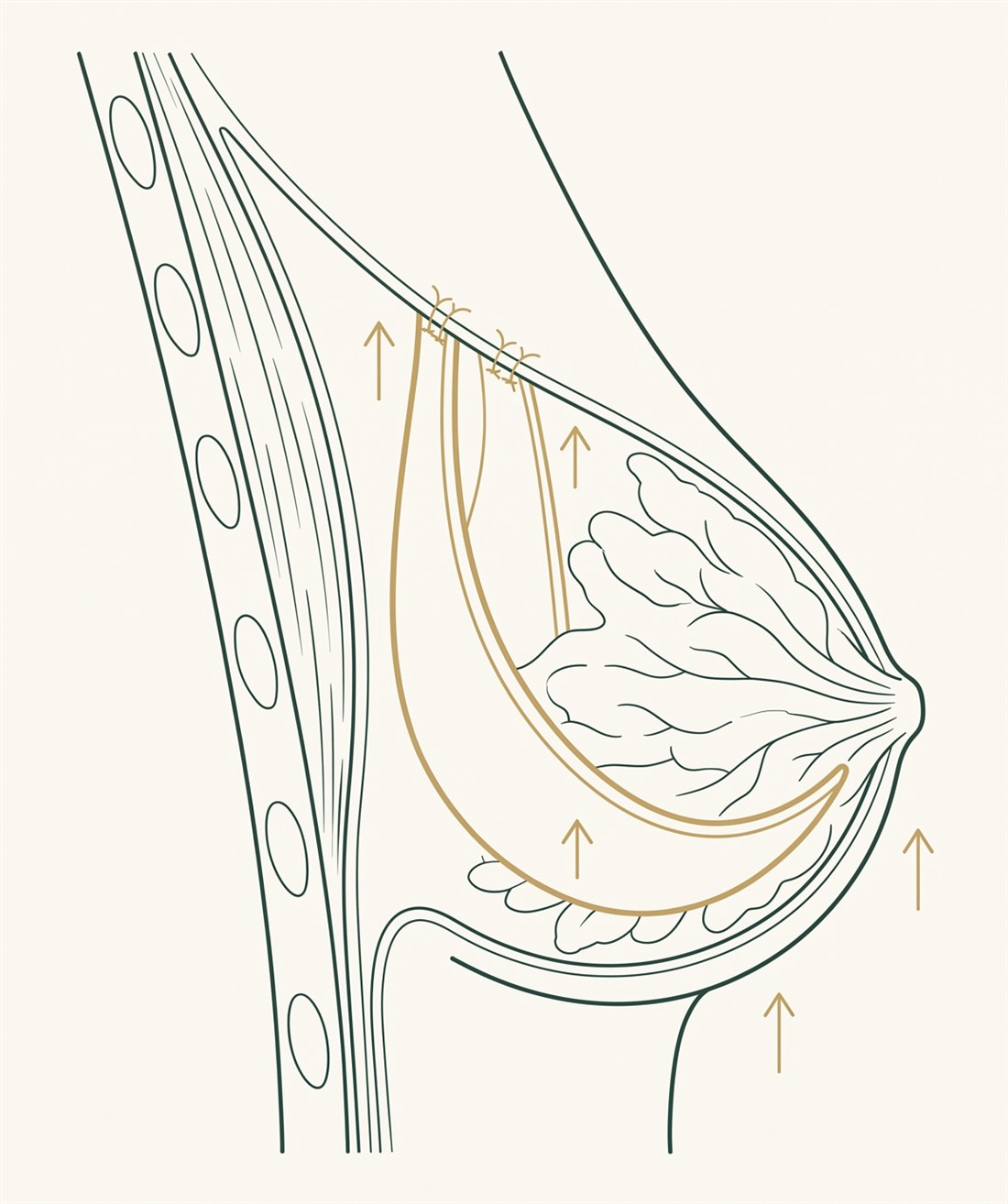
What is the internal bra?
An advanced internal suturing technique that reinforces the breast fold and lower pocket with your own tissue, creating a support that keeps the implant in position long-term. It reduces bottoming out and drift — two of the commonest reasons for revision.
What is hybrid breast augmentation?
A silicone implant combined with fat grafting from your own body. The implant provides volume and structure; the fat softens edges and deepens cleavage. It is ideal for thin patients and for refined, natural transitions.
How painful is it, and how fast is recovery?
With ultrasound-guided nerve blocks and atraumatic technique, most describe tightness rather than sharp pain — like an intense chest workout. Most return to light activities within 24–48 hours, lower-body gym at ~2 weeks and chest training at 4–6 weeks; implants settle over 3–6 months.
Do breast implants need to be replaced every 10 years?
No — that is a myth. There is no mandatory schedule. Implants are exchanged only for a reason (rupture, contracture, size change). They do require surveillance: ultrasound or MRI from about 5–6 years, then every 2–3 years, per FDA guidance.
Can I breastfeed after breast augmentation?
Most women breastfeed normally. The inframammary incision avoids the gland and milk ducts, and dual plane places the implant behind — not inside — the breast tissue. No research has shown silicone implants to be harmful to a nursing infant.
Can I still have mammograms with implants?
Yes. Radiologists use implant-displacement (Eklund) views to image the breast fully. Implants do not cause breast cancer or prevent screening — follow the same schedule as women without implants and inform the imaging team beforehand.
What is capsular contracture?
Tightening of the natural scar capsule around an implant, making the breast feel firm or look distorted. With the modern implant surfaces used here, published rates in primary augmentation are around 1% — versus over 10% with earlier-generation devices.
What is BIA-ALCL, and should I worry?
A rare, treatable lymphoma of the implant capsule associated overwhelmingly with textured implants (estimated 1 in 2,200 to 1 in 86,000 textured-implant patients). The ASPS reports no confirmed cases involving only smooth implants. Surface choice and this evidence are discussed openly at consultation.
Round or teardrop implants — which is better?
Neither universally. Round gives more upper-pole fullness and cannot rotate; anatomical mimics the natural slope. Modern ergonomic implants behave like a teardrop upright and a round lying down. The choice is made from your anatomy and 3D simulation.
Do I need a breast lift with my implants?
If your nipple sits at or below the fold when standing, an implant alone cannot correct the sagging — you need an augmentation-mastopexy (implant + lift). This is assessed with measurements at consultation, and you are always told honestly which operation your anatomy needs.
Can implants correct asymmetry?
Yes — it is a core indication. Options include different implant sizes per side, hybrid fat grafting for millimetric refinement, or a lift on one side only. Perfect symmetry is never guaranteed, but meaningful improvement is the norm.
I had implants placed elsewhere and I’m unhappy — can they be revised?
Yes. Revision augmentation is performed for capsular contracture, malposition, rippling, size change or implant exchange — including complex cases using polyurethane-surfaced implants, which show among the lowest published contracture rates in revision settings.
PM
Medically reviewed by Dr. Paulo Michels
Brazilian-trained plastic surgeon · 18+ years · ISAPS, ASPS, SBCP & EPSS member · advanced training in Germany & the USA · book author & international speaker · Elyzee Hospital, Abu Dhabi · About Dr. Paulo Michels →
Last updated July 2026