Modern anaesthesia
General anaesthesia (TIVA)
Total intravenous anaesthesia gives a safe, deeply comfortable procedure and a smooth, clear-headed wake-up with very little nausea. Most patients go home the same day or after one night.
Migraine Surgery · Abu Dhabi & Dubai
For chronic migraine that no longer responds to medication, surgery can release the compressed nerves at the trigger points that set the attacks off. It is not brain surgery — and in carefully selected patients, published results are striking: most improve, and around half become free of migraine.

Overview
Migraine surgery — nerve decompression, or trigger-site deactivation — treats migraine at its peripheral trigger points. In many patients an attack is set off where a sensory nerve is compressed by a small muscle, blood vessel, band of fascia or a point of contact in the nose. Releasing that pressure removes the trigger.
It is not brain surgery: it addresses small sensory nerves just beneath the skin of the face, scalp and neck, and never touches the brain or the skull. It is usually a day case, through incisions hidden in the hairline, the upper-eyelid crease or inside the nose.
It is not a first step and not for everyone — it is for people with chronic migraine that has not responded to medication, in whom a specific trigger site can be identified and confirmed. Honest, careful selection is the heart of this operation, and Dr. Paulo Michels works alongside your neurologist throughout.
The idea behind it
The peripheral trigger theory — developed and validated over two decades of plastic-surgery research — holds that in many sufferers a migraine begins where an irritated sensory nerve is squeezed at a specific point. Relieve the compression, and the cascade never starts.
At the trigger site, a small muscle, artery, fascial band or nasal contact point presses on and irritates a sensory nerve. That constant irritation is what fires the migraine — which is why the pain so often starts in the same spot every time.
Surgery decompresses the nerve — freeing it from the structure pressing on it. With the irritation gone, the trigger is switched off, so attacks become far less frequent, milder, or stop altogether. It treats the cause at that site, not just the symptom.
The map
Migraines have recognisable patterns depending on which nerve is involved — and identifying your pattern is the whole basis of the operation. A useful sign is pain that reliably starts at one spot you can point to.
Many patients have more than one trigger site; where appropriate the dominant one is treated first, or several are released in the same operation.
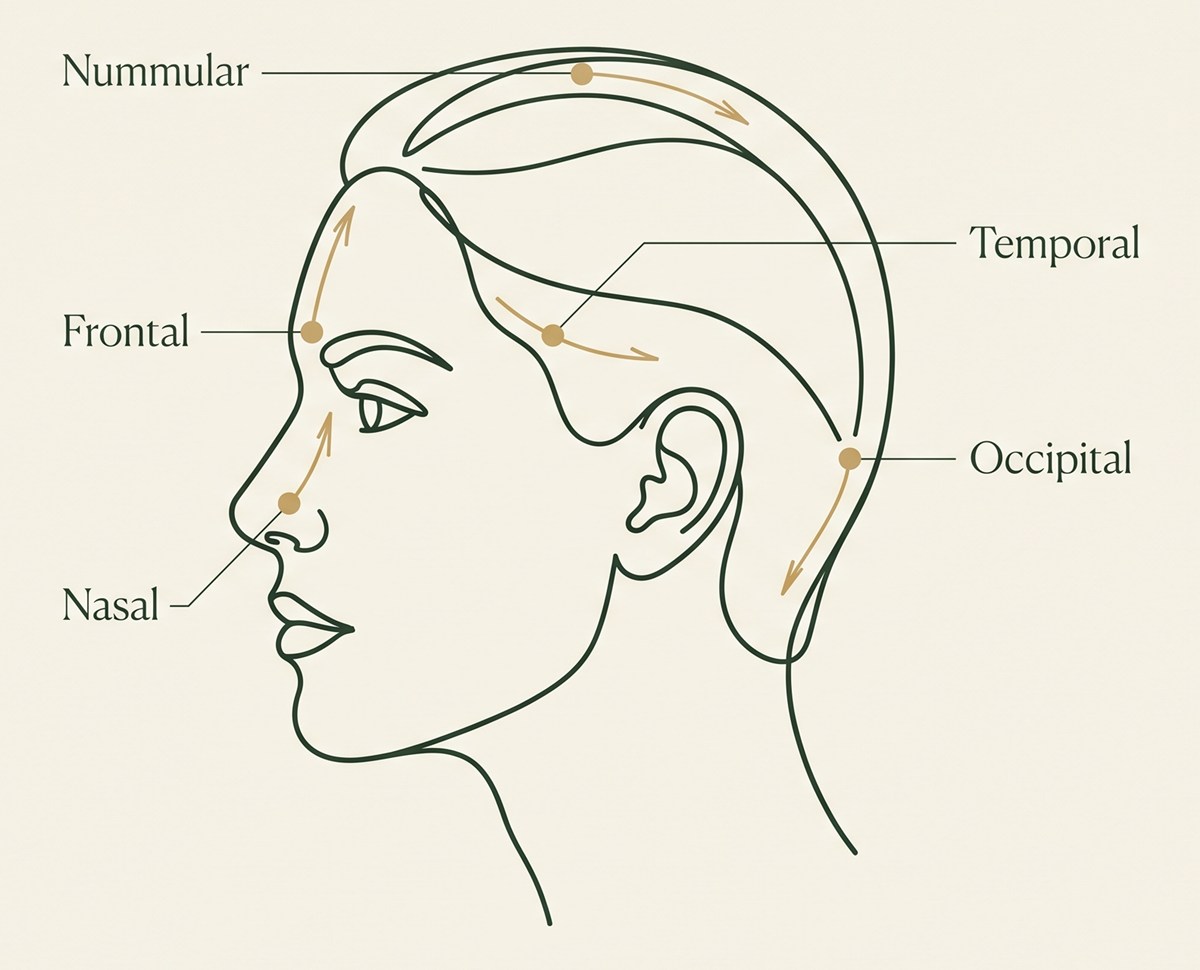
Pain that begins around the eyebrows or between the eyes and spreads across the forehead. The supraorbital and supratrochlear nerves are released from the corrugator muscle — through the upper-eyelid crease or endoscopically.
Sharp, throbbing pain in the temple, at the side of the head above and in front of the ear. The zygomaticotemporal branch is released through a small incision hidden in the hair.
Pain at the base of the skull radiating up toward the crown, often shooting or electric. The greater occipital nerve is freed from the muscle and vessels compressing it — the zone with the most consistent reported results.
Pressure deep behind or between the eyes, mimicking sinus congestion, from contact points inside the nose. Corrected internally by septoplasty and turbinate work — no external scar.
A fifth, less common site
Some patients have a small, coin-shaped tender spot on the top of the scalp that stays consistently in the same place — a nummular trigger. When confirmed, the nerve at that point is released like the others.
The most important step
The success of migraine surgery depends almost entirely on choosing the right patient and the right site. Dr. Paulo Michels never operates on a guess — a confirmatory test is central to deciding whether surgery is appropriate.
Finding the trigger
Candidacy
Honest selection
Just as important is knowing when to say no. Migraine surgery is not appropriate for migraines that begin centrally (within the brain), hormone-driven or vestibular migraines, headaches from unrelated sinus disease, patients who have not yet tried standard treatment, those with no relief from the diagnostic block, unaddressed medication-overuse headache, or where anaesthetic risk is too high. In these cases medication and neurology care remain the right path — and Dr. Paulo Michels will tell you so.

Our philosophy
The evidence
For carefully selected patients, the published results are consistent. Migraine surgery has been studied in peer-reviewed trials over more than twenty years — but results vary between individuals and are never guaranteed.
In published studies of suitable patients, roughly 9 in 10 experience a meaningful reduction in the frequency, intensity or duration of their migraines.
Around half of well-selected patients report becoming completely free of migraine after decompression of the confirmed trigger sites.
Most who respond well reduce their migraine medication, and some stop daily preventives — which can also help medication-overuse headache.
Figures reflect peer-reviewed outcomes of trigger-site deactivation surgery in appropriately selected patients; the occipital zone tends to give the most consistent results, and benefit has been maintained at five years. Results vary between individuals, are not guaranteed, and depend on correct trigger identification — all discussed honestly at your consultation, and medication changes are always made gradually with your neurologist.
Comfort & healing
The procedure is comfortable and designed so the incisions are hidden in the crease of the lid, within the hair, or entirely inside the nose.
Modern anaesthesia
Total intravenous anaesthesia gives a safe, deeply comfortable procedure and a smooth, clear-headed wake-up with very little nausea. Most patients go home the same day or after one night.
Hidden access
The frontal site is reached through the upper-eyelid crease or endoscopically; the temporal, occipital and nummular sites through small incisions hidden in the hair; the nasal site entirely from inside the nose. Incisions are inconspicuous once healed.
A dual benefit
Because the frontal release removes the frown (corrugator) muscle, it also softens the frown lines between the brows — a natural aesthetic benefit alongside the relief.
Book a private consultation with Dr. Paulo Michels — an honest assessment of your migraines, whether a trigger site can be confirmed, and whether decompression surgery is right for you.
Recovery
Recovery is quicker than most expect for a procedure with such lasting benefit. Most people are back to desk work within about a week.
Mild, medication-controlled discomfort. You rest with the head elevated; some bruising around the eyes is expected after frontal work. Nasal work may feel congested.
Many return to light activity and desk work. Any sutures are removed and early swelling settles.
Exercise resumes gradually. Neck stiffness after occipital work eases; some numbness or tightness at the treated site is normal while the nerve settles.
Most people reach essentially full recovery.
The effect on the migraines usually becomes clearer. It is not unusual to have a headache, or even a migraine, in the early days or weeks — this does not mean the surgery has failed. For those who respond, the relief is lasting.
Good to know
Honest risks
Patient stories
“I had migraines fifteen days a month for years. The test block worked, so we operated — I now go months without one. It gave me my life back.”Frontal + temporal
“Mine started at the back of my head and no tablet touched them. He released the occipital nerve and the change has been extraordinary.”Occipital release
“He was honest that I first needed the tests to confirm the site. That care is exactly why the result was so good — and my frown lines softened too.”Confirmed trigger
FAQ
No. It addresses small sensory nerves beneath the skin of the face, scalp and neck, through incisions hidden in the hairline, an eyelid crease or inside the nose, and does not involve the brain or the skull. It is usually performed as day surgery.
A useful sign is pain that reliably starts at one spot you can point to and eases when that nerve is numbed with a test injection. Migraines that begin diffusely or deep inside the head are usually central and not suitable. A neurologist’s diagnosis always comes first.
For carefully selected patients, yes. Published studies of suitable patients report that most improve — roughly 9 in 10 gain a meaningful reduction — and around half become free of migraine, with benefit maintained at five years. Results vary between individuals and are not guaranteed, which is why confirming the trigger site beforehand matters so much.
It is not described as a guaranteed cure, and it is not for every migraine sufferer. For people with a confirmed peripheral trigger who have not responded to medication, it can dramatically reduce or eliminate attacks. For others, medication and neurology care remain the right path.
The main four are frontal (forehead and between the brows), temporal (the temple), occipital (the back of the head and neck) and nasal or rhinogenic (contact points inside the nose). A fifth, less common site is nummular — a coin-shaped tender spot on the top of the scalp. Each involves a specific nerve, and many patients have more than one.
Many patients who respond well reduce their medication and some stop daily preventives, which can also help medication-overuse headache. This varies and is not guaranteed, and any changes are made gradually with your neurologist — prescribed medication should never be stopped on your own.
They are different. Botox for migraine relaxes muscle temporarily and is repeated periodically; nerve decompression aims to give longer-term relief by releasing the nerve. Here, Botox is used mainly as a diagnostic test — a positive response predicts that surgery on that nerve will work.
No obvious ones. The frontal site is reached through the upper-eyelid crease or endoscopically, the temporal, occipital and nummular sites through small incisions hidden in the hair, and the nasal site entirely from inside the nose. Some bruising around the eyes is expected after frontal surgery and settles within a couple of weeks.
Mostly temporary effects — numbness near the nerve, some temple hollowing, neck stiffness, or nasal dryness depending on the zone treated. Where a nerve is divided rather than released, a small area of numbness can be permanent. Serious complications such as infection or bleeding are uncommon, and general anaesthetic risks also apply.
Most people return to desk work in about a week and to fuller activity by 4–6 weeks, with the effect on migraines usually clearer by around three months. Early post-operative headaches can occur and do not necessarily indicate failure.
This may reflect an unsuitable candidate, a hidden second trigger zone, or an incomplete release. The latter two can sometimes be addressed by treating the additional zone or by revision; the first is unlikely to benefit from further surgery. These possibilities are discussed openly before any decision.
It can, but fasting and altered sleep can affect early healing and migraine patterns, so the timing is best planned with your surgeon.
Enquiry
Leave your details and Dr. Paulo Michels’ team will reply personally — or message on WhatsApp.